Muhammad Salman1,2,
Naureen Shehzadi1,
Muhammad T Khan3,
Muhammad Islam1,
Sohail Amjad1,
Omer Afzal1,
Sibghat Mansoor1,
Shaista Qamar1,
Sohaib Peerzada3,
Amer H Khan2,
Khalid Hussain1 ![]()
For correspondence:- Khalid Hussain Email: khussain.pharmacy@pu.edu.pk Tel:+924299211617
Received: 11 May 2015 Accepted: 12 March 2016 Published: 30 April 2016
Citation: Salman M, Shehzadi N, Khan MT, Islam M, Amjad S, Afzal O, et al. Erectile dysfunction: prevalence, risk factors and involvement of antihypertensive drugs intervention. Trop J Pharm Res 2016; 15(4):869-876 doi: 10.4314/tjpr.v15i4.29
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To explore the literature regarding prevalance, risk factors and the involvement of antihypertensive drugs in erectile dysfunction (ED).
Methods: Original research articles, reviews, editorials and case reports published in English language on the prevalence of sexual/erectile dysfunction in hypertensive men taking antihypertensive drugs and risk factors were identified through a search of four bibliographic databases, namely, PubMed, EMBASE, CINAHL and EBSCO Health.
Results: Recent analyses suggest that hypertensive men of almost all age groups suffer from ED but it is more prevalent in elderly male patients. The involvement of β-blockers was found to be controversial. Nevertheless, some evidence had been found regarding the use of propranolol in high doses.
Conclusion: The present review indicates the need for research to unravel the role of β-blockers in the manifestation of ED in hypertensive males, whom there are no contributory factors such as sedentary lifestyle, aging, stress and anxiety, etc.
Introduction
Hypertension (blood pressure > 140/90 mm Hg) is managed by a number drugs of different pharmacological groups. The treatment often requires the use of multiple drugs in combination. However, antihypertensive drugs such as diuretics, potassium sparring diuretics and β-blockers are believed in to be involved in erectile dysfunction (ED) [1,2]. ED refers to diminished libido, erectile failure (inability of achieving and/or maintaining sufficient penile erection for intercourse) and different types of ejaculatory problems [3]. This disorder has a negative impact on lowering blood pressure [4-6]. The fear of ED and its manifestation leads to emotional disturbances and noncompliance to the therapy, thus affecting patient’s health [7,8]. Therefore, the present article focused in exploring the facts regarding the prevalence, risk factors and involvement of antihypertensive drugs. The literature review indicated several reports about a significant prevalence of the dysfunction in normal population.
The present review of literature was carried out to respond to the question, ‘are there any clear, demonstrable and meaningful relationship between the use of antihypertensive drugs and manifestation of ED’? By doing so, we wish to examine and assemble the available evidence regarding the role of antihypertensive drugs, particularly β-blockers in manifestation of ED. Additionally, by uncovering the underlying causes of ED and exploring the mechanisms by which antihypertensive drugs manifest this disorder, we may provide information to healthcare providers for selecting drugs, having safer profile and appropriate dose. This article may certainly leave a beneficial impact on clinical and pharmaceutical care practices involved in effective management of hypertensive patients who are high risk for ED.
Methods
Search strategy
A literature search was conducted on PubMed, EMBASE, CINAHL, ProQuest and EBSCO Health databases to find all potentially relevant publications. The key words used for search include: “antihypertensive agents”, “sexual dysfunction”, “erectile dysfunction”, “β-blockers” and “risk factors”. The reference lists of primary original articles and review articles were also review so that further relevant studies could be taken into account.
Study selection
Research articles, reviews, editorials, and case reports published in English language regarding the use of antihypertensive drugs, particularly β-blockers, and the manifestation of ED were included, and the data was then published as opinions, commentaries and conference abstracts were excluded due to the insufficiency of information.
Data extraction
One investigator reviewed the papers to evaluate potential relevance. The data were drawn from the included studies to identify the results of investigations indicating the relationship between antihypertensive therapy, particularly β-blockers, and ED. Additionally, descriptive features and data analysis methods were identified that could indicate the strength of evidence. The risk factors, comorbidities and ED mechanism of antihypertensive drugs were also extracted.
Results
Prevalence of erectile dysfunction (ED)
The normal population was also found to be suffering from ED. A study indicated that twenty six person per one thousand were found to suffer from ED [9]. Another study indicated that more than half of the men's population (52 %), aged 40 - 70 years, were suffering from some degree of ED [10]. An interview-based study conducted by psychologist involving 98 sexually active men, aged 20 - 35, shows that 8.25 % of the respondents reported ED during intercourse and 18.50 % during masturbation [11]. In addition, a study conducted on matrimonially stable couples, men age (37.42 ± 11.15 years) and women age (35.04 ± 10.07 years), indicated that 7 % men failed in achieving an erection and 9 % could not maintain erection [12].
Risk factors
ED was found in almost all age groups but the incidences were higher in elderly men. A study indicated the prevalence of 2 %, 6.7 % and 24 % in respondents aged ≤ 40, 55 and 70 years [13]. A similar relationship was revealed in another study, in which the prevalence was 1 - 10 % in younger males (< 40 years), 2 – 9 % in middle age (40 - 50 years), 20 – 40 % in older people (60 - 69 years) and 50 – 100 % in elderly people (> 70 years) [14].
A German population-based study indicated that 19.2 % ED surged was related to age ( 2.3 - 53.4 %) and comorbidities like hypertension and diabetes [15]. A Turkish population-based study indicated 69.2 % age-adjusted overall incidence of ED with varying degree of severity (33.2 % mild, 27.5 % moderate and 8.5 % severe) [16]. This study further indicated that age, lower education, unemployment, hypertension, diabetes and depression were the contributing factors for ED [16]. An age-adjusted prevalence of ED in Brazil, Italy, Malaysia and Japan was reported to be 15 %, 17 %, 22 % and 34 %, respectively [17]. These populations also indicated aging, heavy smoking, cardiac diseases and diabetes were the other risk factors [17]. A Tampere Ageing Male Urological Study indicated the relationship of the dysfunction with age (mean score increase from 0.82 (50 years) to 1.85 (75 years), hypertension (r = 5.1), cardiac diseases (r = 6.5), diabetes (r =17.5) and smoking (r = 4.6) [18]. An Italian study indicated prevalence (19.9 %) and other factors as: higher age (4.6 % in male < 25 years, 37.65 in male > 74 years), diabetes (Odds ratio (OR) 1.2, 95 % Cl 1.1 - 1.4), hypertension (OR 1.3, 95 % Cl 1.1 - 1.4) and cardiopathy (OR 1.5, 95 % Cl 1.3 - 1.8) [19]. A study involving 2869 men in Vienna indicated 32.2 % prevalence of ED and high risk contributors; diabetes (OR 3.0, 95 % Cl 1.53 - 5.87), hypertension (OR 2.05, 95 % Cl 1.61 - 2.6), hyperlipidemia, stress and sedentary lifestyle [20].
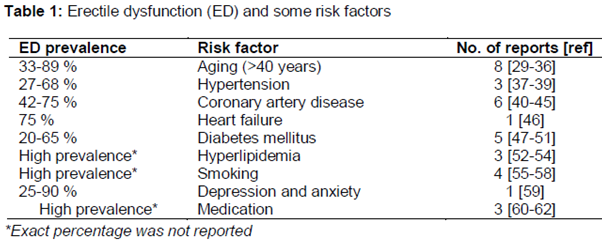
The first large study to explore the prevalence of sexual dysfunction in hypertensive subjects “Treatment of Mild Hypertension Study” indicated that this disease was considerably low in females (4.9 %) compared to males (14.4 %) [21]. However, in this study, mild-hypertensive patients and patients of 45 - 69 years were included, whereas severe-hypertensive, diabetic and elderly patients (> 70 years) were excluded, and only one question was used to assess the disease [21]. A study carried out on 2130 hypertensive Spanish men indicated 45.8 % prevalence, whereas it was 18.5 % in the general population [22]. Similarly, a study involving 634 Greek men indicated that 35.2 % hypertensive subjects and 14.1 % normal subjects suffered from ED [23]. The manifestation of ED was said to be more common in hypertensive population compared to that of the normotensives [21-24]. A number of studies showed that ED shared many risk factors of the cardiovascular diseases such as atherosclerosis [25], hypertension, hyperlipidemia, diabetes mellitus [26], smoking [27], obesity and inactive lifestyle [28]. The prevalence of ED in the presence of different comorbidities is summarized in .
Etiology of ED in hypertensive patients and probable mechanism
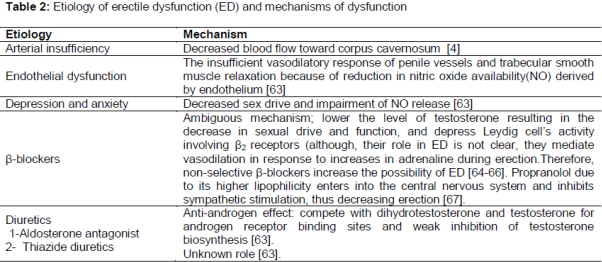
The etiologies of ED in hypertensive patients are almost similar to that of the general population. There are several social, psychological, physiological and drug-related effects that can enhance the incidence of the disease. However, based on the literature review, etiologies of the dysfunction and probable mechanisms by which antihypertensive drugs manifest ED are shown in .
Antihypertensive drugs and ED
The summary of the literature reported regarding the involvement of antihypertensive drugs particularly β-blockers in ED, study design, sample size, drugs used and the major findings is given as follows:
The literature has numerous reports regarding the relation between ED and β-blockers. A multicenter, randomized, placebo-controlled trial, recruiting 697 hypertensive patients (21 - 65 years), taking atenolol and chlorthaildone indicated that ED was severe in 11 % participants [68]. A prospective, randomized, double blind study, conducted on 192 men suffering from coronary heart disease, indicated that sex life of the subjects was not affected by using metoprolol, because ED scores remained the same in the drug and placebo groups. Around 60 % of the study population had no complaints regarding erection and reaching orgasm [69].
The effect of carvedilol and valsartan (angiotensin-receptor blockers) on sexual activity and plasma testosterone was compared in a randomized, double blind, crossover study, recruiting 160 hypertensive men (40 - 49 years), indicated ED in 15 patients taking carvedilol (13.5 %), and 1 patient each taking valsartan and placebo [70]. In another double blind, parallel arm study, conducted on 110 hypertensive men (age 40 - 49 years), using valsartan and atenolol to evaluate their role on sexual activity and testosterone levels indicated that atenolol significantly reduced sexual activity (from 6.0 episodes of sexual intercourse/month to 4.2 episodes/month vs placebo, p < 0.01), whereas valsartan significantly improved sexual function compared to atenolol (p < 0.05), but the effect was not significant compared to placebo (p = 0.058) [71]. Silvestri et al [72] carried out a two phase study - first phase parallel study and second double blind, placebo-controlled, single crossover study on 96 men (40 % with angina and 60 % hypertension), aged (52 ± 7 years), who were well-informed about sexual side effects of atenolol and it had been indicated that ED incidences were only 3.1 % in a group not knowing the drug, 15.6 % in a group knowing the drug and 31.2 % in a group aware of the side effects of the drug.
A placebo-controlled study involving 134 hypertensive males using Propranolol and Chlorothiazide revealed 11 % cases of impotence and 7 % failed ejaculation in propranolol group, 14 % impotence and 5 % failed ejaculation cases in placebo group and 10 % impotence and 6 % failed ejaculation cases in untreated hypertension group [73]. A multicenter, randomized, double blind, clinical trial on 626 mild to moderate hypertensive men using drugs such as captopril, methyldopa, propranolol and hydrochlorthiazide indicated that the participants taking captopril raised less complaints of ED than those taking propranolol [74]. Two case reports in the year 1976 indicated that ED in hypertensive patients was caused by the use of propranolol [75,76]. Warren et al [77] reported 5 % incidence of sexual dysfunction in a prospective follow-up study on 63 patients (49 men and 11 women) suffering from angina prectoris and being treated with Propranolol. In another independent study, the same authors reported that 5 % incidence of ED was due to the use of propranolol [78]. A randomized, double blind, crossover study which recruited 40 hypertensive male patients showed that 18 % cases of impotence and 27 % diminished libido were in a group consuming propranolol at a dose of 320 mg/day [79].
Two further reports were found which indicate that propranolol-induced ED is dose-related. The first study [80] conducted on 46 patients with no prior ED indicated 15 % cases of complete erectile failure (getting mean daily dose of 143 mg/day) and 28 % cases of decrease in quality of erection (receiving mean daily dose of 124 mg/day) and in the second study [79] participants receiving a dose of 180 - 320 mg/day suffered from complete erectile failure or decreased potency, while 57 % of those treated with 120 - 160 mg/day reported other complaints similar to that of the first study. Interestingly, patients taking a mean daily dose of 83 mg/day of propranolol did not report any incidence of ED [80].
Moreover, in the study of Holliefield et al [79] not even a single person out of 40 subjects, consuming propranolol 160 mg/day, complained of ED; only 2 persons out of 11 (18 %) reported complete erectile failure/impotence (taking a dose of ≥ 320 mg) and 3 out of 11 (27 %) reported a decreased sexual desire. Only one study addressed the effect of propranolol upon ejaculation and this study revealed 7 % incidence of failed ejaculation in hypertensive subjects [73]. On the other hand, 6 % of the general population, 10 % untreated group and 5 % taking placebo, reported the same problem. Hence, there was very little support regarding the effects of propranolol on ejaculation.
Discussion
The results of this literature survey were stunning in a number of aspects. Firstly, the reported literature did not support the involvement of β-blockers in the manifestation of ED. Secondly, we did not find even a single study conducted on retrospective data regarding β-blockers-induced ED. Almost all of the studies were prospective. Its probable cause may be the unavailability of sufficient data in the patient’s record needed to draw conclusions about the involvement of β-blockers in the manifestation of ED. Furthermore, hypertensive patients taking β-blockers may suffer from ED because of psychological factors (depression, stress, anxiety, loss of relation and known side effects of drugs), co-morbidities, adjuvant medication, heavy smoking, obesity and sedentary lifestyle. On the other hand, in this literature survey, we found concrete evidence regarding the involvement of propranolol in the manifestation of ED.
However, we did not find any clear mechanism which suggested that propranolol caused the disease. The involvement of atenolol and carvediolol in manifestation of ED was controversial, since only one study indicated that carvedilol had a negative impact on sexual function [70]. Two studies [68,71] revealed that ED was caused by atenolol; in the first [68] the difference between the two groups, receiving atenolol and usual diet and those receiving placebo and usual diet was not statistically significant (p > 0.05). Contrary to the findings of second study [71], Silvestri et al [72] reported that the incidence of ED was very high in those subjects who were well-informed regarding sexual side effects of atenolol than those unaware of the given antihypertensive agent (31.2 vs 3.1 %).
These findings indicate that awareness of the patients regarding the side effects of the drug played a contributory role in the manifestation of this disorder [72]. In addition, anxiety, stress and fear were also reported to be involved in causing sexual dysfunctions [81]. Numerous studies suggest that anxiety is common amongst sufferers of sexual dysfunctions, with varying levels and nature of anxiety and anxiety reduction procedures improve some aspects of sexual dysfunctions [80]. It is suggested that the knowledge of side effects produce anxiety that may affect sex life or erectile function [72]. Therefore, further investigations are required in order to understand and clarify the role of β-adrenergic receptor antagonists in causing erectile dysfunction.
Conclusion
Erectile dysfunction (ED) is a widespread problem among the hypertensive male population and it adversely affects both patient’s quality of life and adherence to treatment regimen. The reported data do not support the conventionally held belief that β-blockers induce ED. However, it was evident that the involvement of propranolol, if used in higher doses, could cause ED and induce ejaculatory disturbances. The etiology of ED in hypertensive males is multifactorial and may be caused by vascular disease, decreased heart capacity, medications and/or other factors such as heavy smoking, psychological issues, obesity and physical inactivity.
References
Archives


News Updates